
Your MRI Is a Snapshot of a Moving Process, Not a Verdict
You get the MRI back and the report reads like an inspector condemning a house. Disc desiccation at L4-L5. Broad-based posterior bulge. Loss of disc height. Annular fissure. You read it on your phone between meetings, and your stomach drops, because it finally sounds like the reason your back has been running your calendar.
Here is the part nobody prints on the report. That same paragraph describes most people your age who feel nothing at all.
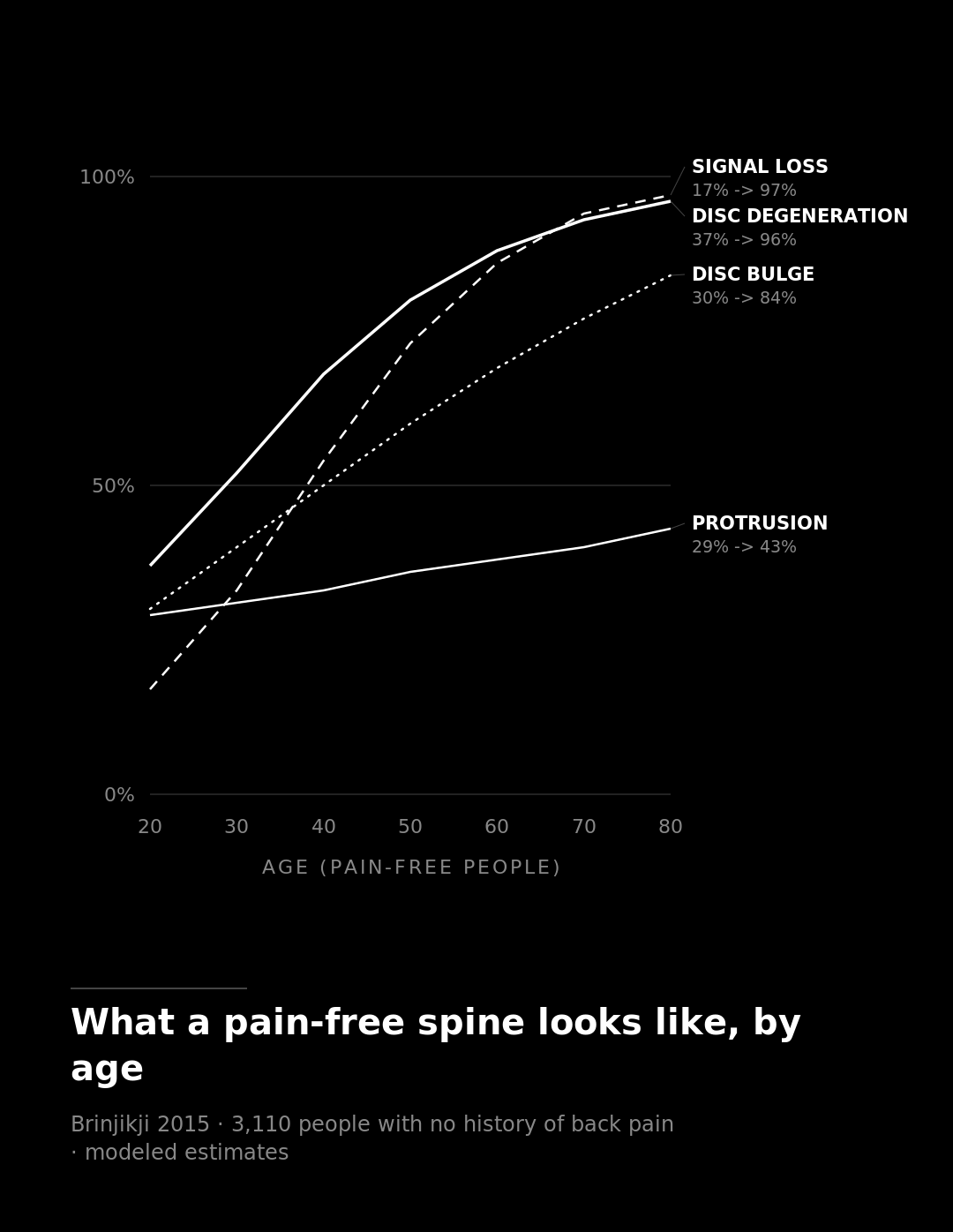
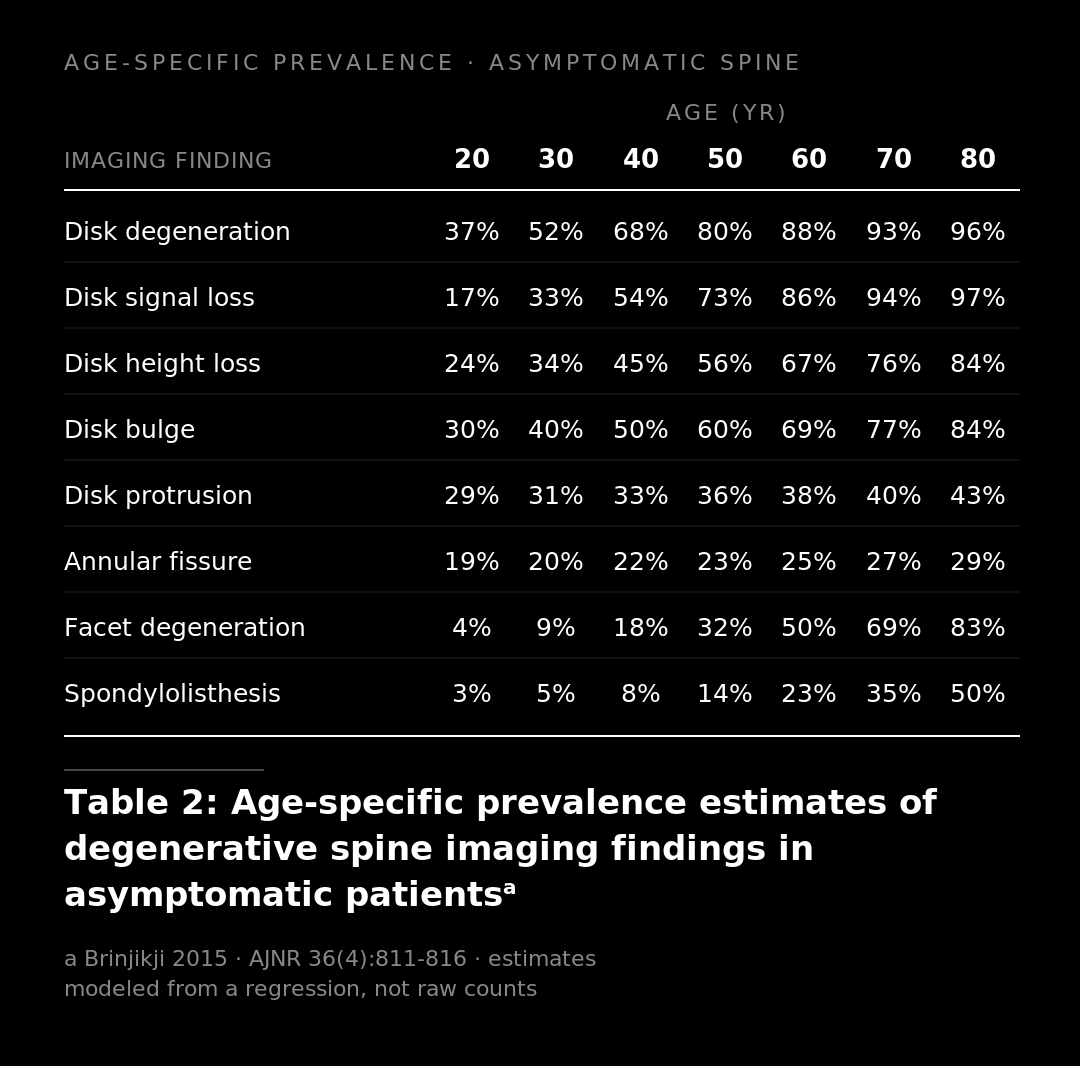
In 2015, a group led by Brinjikji pooled 33 imaging studies covering 3,110 people with no history of back pain and modeled how common these findings are by age. At 20, roughly a third of pain-free people already show disc degeneration. By 50, it is around 80%. By 80, it is nearly everyone. Signal loss, height loss, bulging, the whole vocabulary of a frightening report climbs the same curve. Half of pain-free people in their thirties already have degeneration, height loss, or a bulge sitting on the film. These are modeled estimates rather than raw head counts, but the direction is not subtle. By the time you are old enough to afford a good MRI, a worn-looking disc is closer to the baseline than the exception.
A smart reader pushes back here. Fine, degeneration is everywhere, but I have a herniation. That is a different thing.
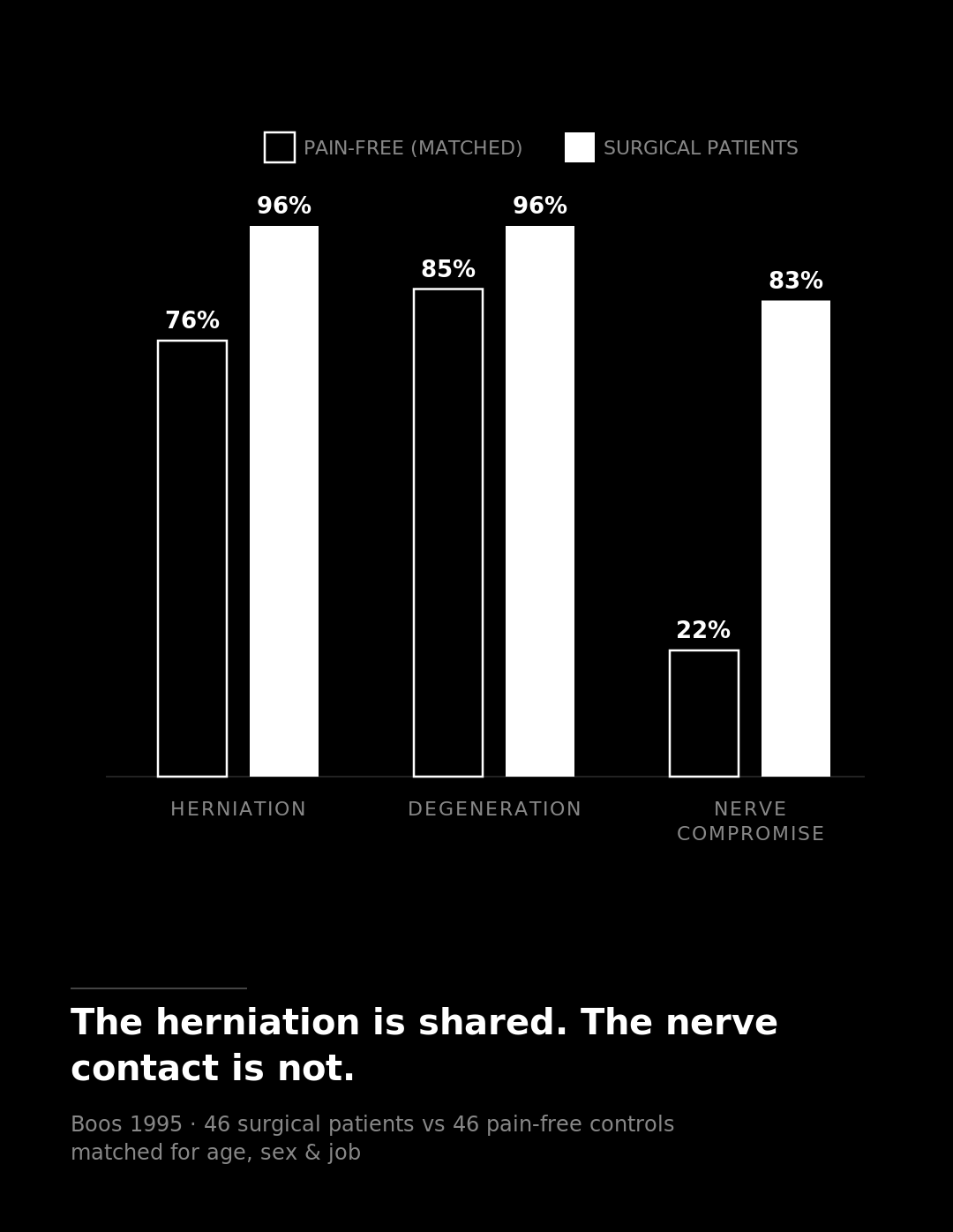
This is where the best study in the literature does something the others do not. In 1995, Boos took 46 people with sciatica bad enough to need surgery and matched each one to a pain-free volunteer of the same age, sex, and job, including the heavy lifting and the desk time you would expect to matter. Then a blinded radiologist read all 92 scans.
Three out of four of the pain-free, matched controls had a disc herniation. 76%. Not a bulge, a herniation. The surgical patients came in at 96%. The herniation itself barely told the two groups apart. Degeneration did not separate them either: 96% in patients, 85% in the pain-free controls, statistically a wash.
So if the herniation sits in both lineups, what actually sorted them? One thing did the heavy lifting: whether the disc was touching a nerve. Nerve root compromise showed up in 83% of the patients and 22% of the pain-free controls. That is the discriminator. And even that was not the whole story. The model that best predicted who was in pain combined the nerve contact with the person's life: work stress, depression, marital strain. Morphology alone, the thing the report shouts about, was a weak classifier.
The same researchers then followed a group of pain-free people who already had abnormalities on their scans, most of them herniations, for about five years. The herniations did not meaningfully get worse. What predicted who ended up seeking treatment or missing work was not the disc on the film. It was the physical demand of the job and the psychosocial load around it. The scan was the weaker predictor of trouble. Sit with that. An imaging study produced a biopsychosocial result.
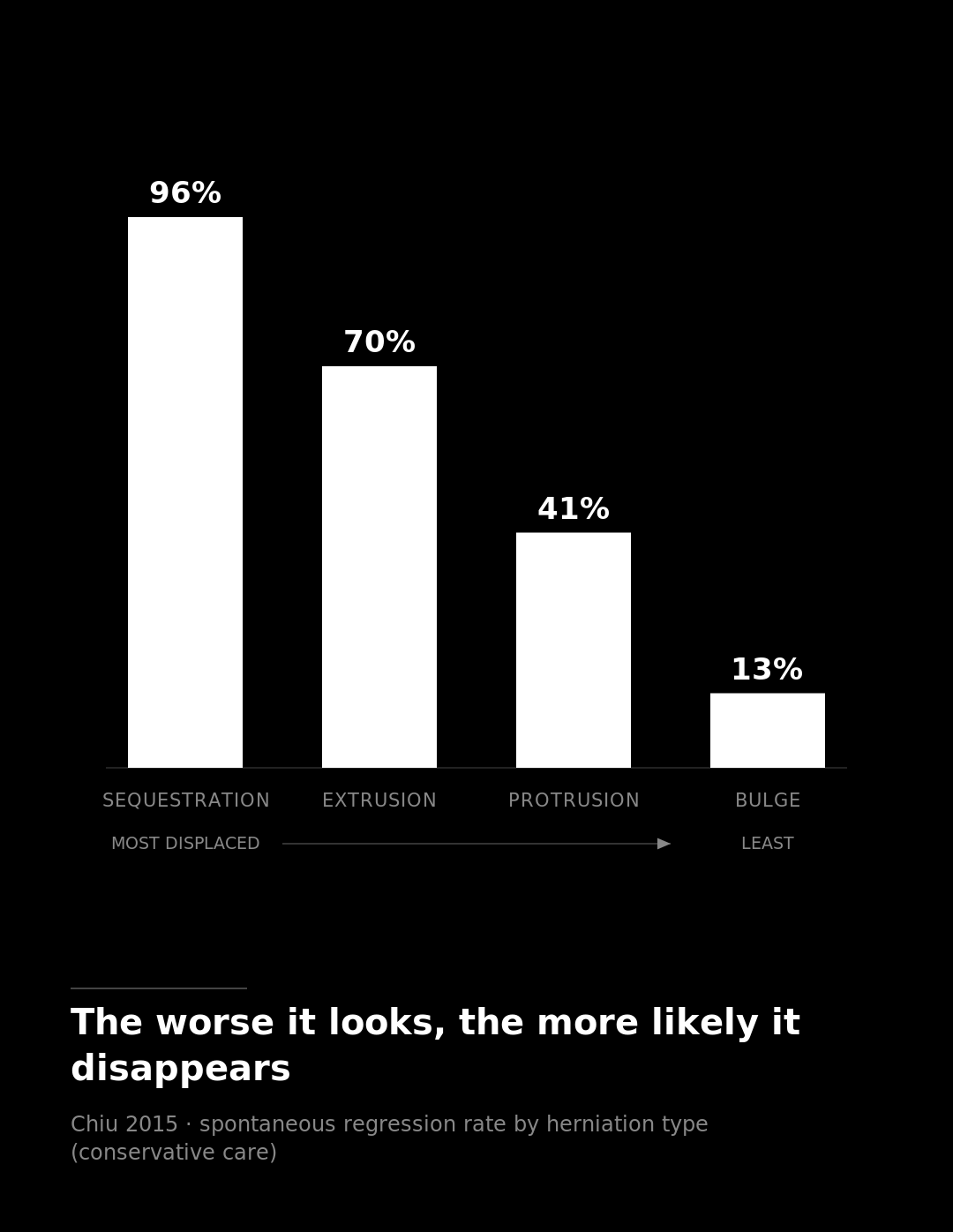
And here is the part that runs exactly backwards from the fear. The bigger and uglier the herniation looks, the more likely your body clears it on its own. A 2015 review by Chiu pooled the regression rates by type. A sequestration, the worst-looking one, where a fragment has broken off entirely, regresses 96% of the time and fully resolves in 43%. An extrusion, the next tier down, regresses about 70% of the time. The mild bulge, the thing that sounds harmless? 13%.
The reason is almost poetic once you see the mechanism. When a fragment breaks loose and meets the bloodstream, the body treats it like foreign debris. Immune cells move in, new vessels grow toward it, and enzymes break the tissue down and haul it off (Yu, Cunha, Kobayashi). The inflammation lighting up the nerve and making you miserable is the same crew that demolishes the herniation. The fragment that is most displaced, most exposed, most alarming on the report, is the one most accessible to that cleanup. The body sends its crew to the loudest wreck first.
Now I have to be honest, because the overcorrection is its own kind of wrong. Resorption is not universal. One three-dimensional volume study watched discs shrink at 35 levels and actually grow at 21 (Seo). More telling, in that study the volume change did not track how people felt. They improved on conservative care whether or not the disc on the film cooperated. Herniations carrying Modic changes, a specific endplate signal, resorb poorly and respond less well (Shan). And degeneration is not pure noise: at the population level it does correlate with pain (Cheung), and severe changes low in the lumbar spine do skew toward the symptomatic side under 60 (Jamaludin).
So the honest stance is not that imaging is meaningless. It is narrower and more useful than that. Imaging findings are common, weak on their own, and only mean something when they line up with the exam and the story. A finding that matches where it hurts and what the nerve test shows is worth attention. A finding sitting at a level that has nothing to do with your symptoms is noise dressed up as a diagnosis.
The report you read between meetings is a single frame pulled from a film that is still rolling. It was taken on the structure's worst-looking day, and your body has very likely already sent the crew in. The scan describes what your spine looked like the morning you lay in the machine. It is not the verdict on what your back can do, and it is the weakest witness in the room to why it hurts.
*This article is educational and not a substitute for medical advice. Consult a qualified professional before making decisions about your health.
Sources
Brinjikji W, Luetmer PH, Comstock B, et al. 2015. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol 36(4):811–816. (Source for the age-by-age prevalence of degeneration, signal loss, height loss, and bulging in pain-free people; the "describes most people your age" claim and the modeled 37%-at-20 to ~96%-at-80 figures.)
Boos N, Rieder R, Schade V, et al. 1995. The diagnostic accuracy of magnetic resonance imaging, work perception, and psychosocial factors in identifying symptomatic disc herniations. Spine 20(24):2613–2625. (The matched-control study: 76% herniation in pain-free controls vs 96% in patients, degeneration a wash, nerve root compromise 83% vs 22% as the discriminator, and the combined nerve-plus-psychosocial predictive model.)
Boos N, Semmer N, Elfering A, et al. 2000. Natural history of individuals with asymptomatic disc abnormalities in MRI: predictors of low back pain–related medical consultation and work incapacity. Spine 25(12):1484–1492. (Five-year follow-up showing herniations did not significantly worsen and that job demand and psychosocial load predicted future consultation and work incapacity better than the disc findings.)
Chiu CC, Chuang TY, Chang KH, et al. 2015. The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clin Rehabil 29(2):184–195. (Regression rates by herniation type: sequestration 96% / full resolution 43%, extrusion ~70%, protrusion 41%, bulge 13%.)
Yu P, et al. 2022. Characteristics and mechanisms of resorption in lumbar disc herniation. Arthritis Res Ther. (Macrophage infiltration, inflammatory response, matrix remodeling, and neovascularization driving reabsorption.)
Cunha C, et al. 2018. The inflammatory response in the regression of lumbar disc herniation. Arthritis Res Ther. (The inflammation implicated in nerve irritation is the main driver of regression and a favorable prognostic sign.)
Kobayashi S, et al. 2009. Ultrastructural analysis on lumbar disc herniation. Spine. (Capillary invasion and monocyte-derived macrophages with collagen-degrading enzymes break down herniated tissue.)
Seo JY, et al. 2016. Three-dimensional analysis of volumetric changes in herniated discs. Eur Spine J. (Honesty hedge: volume decreased at 35 levels but increased at 21, and volume change did not correlate with clinical outcome.)
Shan Z, et al. 2014. Spontaneous resorption of lumbar disc herniation is less likely when Modic changes are present. Spine. (Modic-change herniations contain less nucleus pulposus and less neovascularization, resorb poorly, and respond less well to conservative care.)
Cheung KMC, et al. 2009. Prevalence and pattern of lumbar MRI changes in 1043 individuals. Spine. (Counterweight: positive population-level correlation between degeneration score and back pain.)
Jamaludin A, et al. 2023. ISSLS Prize in Clinical Science 2023. Eur Spine J. (Severe degeneration skews symptomatic only at lower lumbar levels and only under 60; degeneration minimal in ~30% of symptomatic people under 50.)