
The Tendon Only Reads One Number
The most-shared tendon advice of the last decade is a 45-second isometric hold. Load the knee, hold it, feel the pain switch off for a while, go play. It spread because it works in the room. You do it, the pain drops, you believe it. That belief was built on two studies out of one lab. The first had six volleyball players in it. The second had twenty.
Then everyone else tried to repeat it. A trial of 91 people with Achilles pain ran isometrics against isotonics against just resting, and none of them produced a meaningful drop in pain. A patellar crossover found the same nothing, a 0.9-out-of-10 change that was no better from isometrics than from regular reps. A plantar fascia trial put isometrics against walking and got a tie, no difference either way. The systematic review and the network meta-analysis both landed in the same place: isometrics are not special for tendon pain. They relieve pain about as well as any other contraction, which is to say sometimes, for some people, for about as long as the warm feeling after any hard set lasts.
So the isometric pain trick isn't a trick. It's just exercise, and exercise sometimes quiets a cranky tendon for an hour. Fine. Useful even. But it was never the thing that changes the tissue, and somewhere along the way people started treating "my pain dropped" as "my tendon healed." Those are different events. They can happen years apart.
Here's what was happening while everyone argued about pain. A group in Berlin was running a cleaner question: not "what feels better" but "what actually remodels the tendon." Their design is the part I love. Same person, one leg trained at low strain, the other leg trained at high strain, everything else matched. Fourteen weeks. The high-strain leg got stiffer, denser, thicker. The low-strain leg, attached to the same human, eating the same food, sleeping the same hours, did nothing. Not a little. Nothing beyond what walking around already gave it.
That's the finding the whole field should be built on. A tendon keeps a running record of the hardest pull you've put through it lately, and it only renovates when you beat that record. Walking doesn't beat it. Easy reps don't beat it. There's a floor, and it sits above the strain of everyday walking, up in the four-to-five-percent range the high-strain leg hit. Everything under that floor reads to the tendon as a Tuesday. No reason to change.
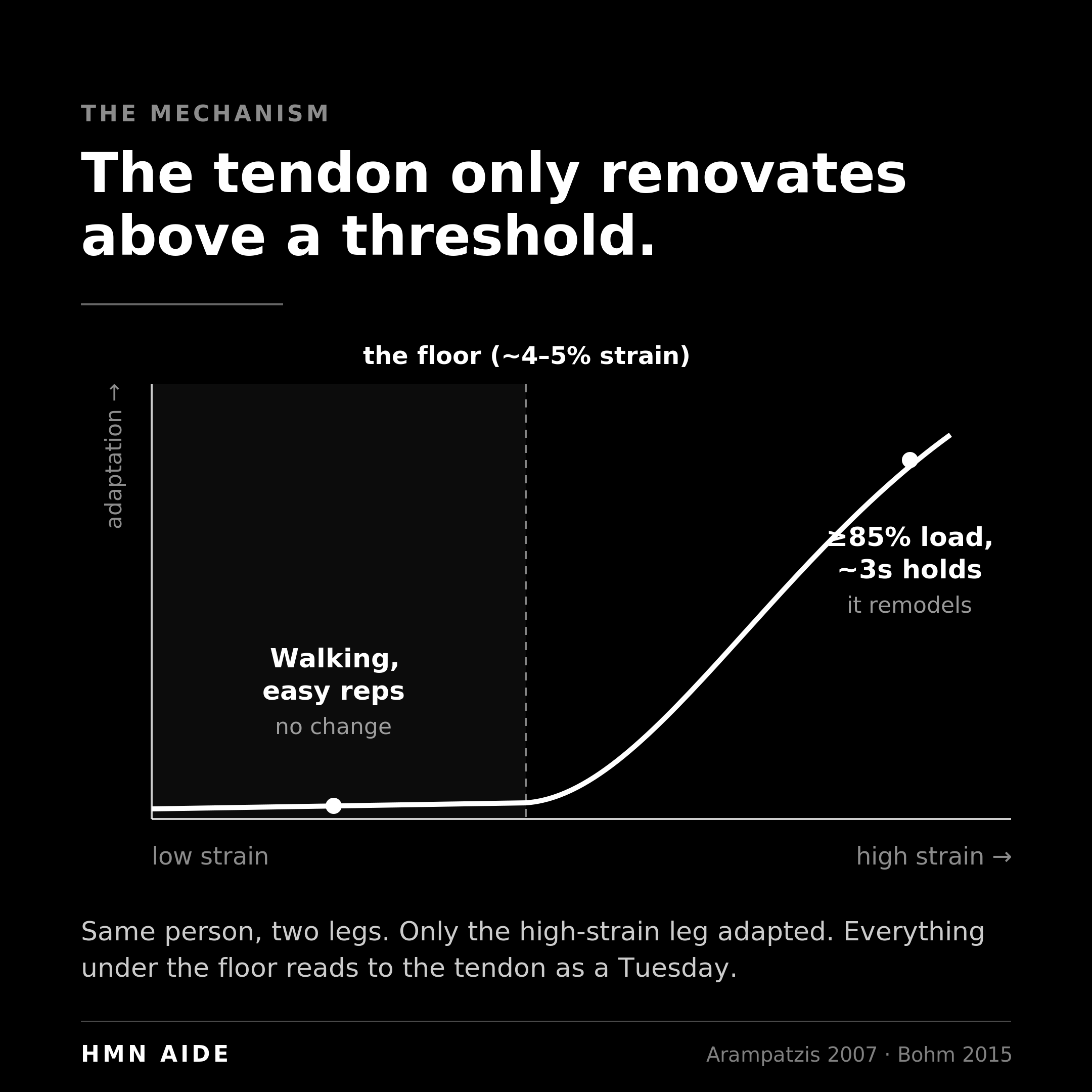
The load that clears the floor is high. The Berlin lab's own training document, written by the people who ran the studies, says it plainly: at least 85 percent of your maximum, held about three seconds, five sets of four, four times a week, for at least three months. Not 60 percent. Not "to tolerance." Eighty-five and up. I pulled their actual PDF to check, because the version floating around coaching circles had softened the number to something more comfortable, and the softening is exactly the problem. People are doing real rehab at well below the required intensity and wondering why the tendon won't turn over.
The other thing the Berlin work settled: contraction type doesn't matter. Eccentric, concentric, isometric, the tendon can't tell them apart and doesn't care. Their meta-analysis of 27 studies found loading magnitude drove the adaptation and contraction type didn't move it. So the decade of "you must do slow eccentrics, only eccentrics" was loading dogma built on nothing. Pick whatever lets you put 85 percent through the tissue and hold it. The contraction is a delivery truck. The tendon only signs for the strain.
Now the parts that are genuinely still open, because pretending they're settled is its own kind of dishonesty.
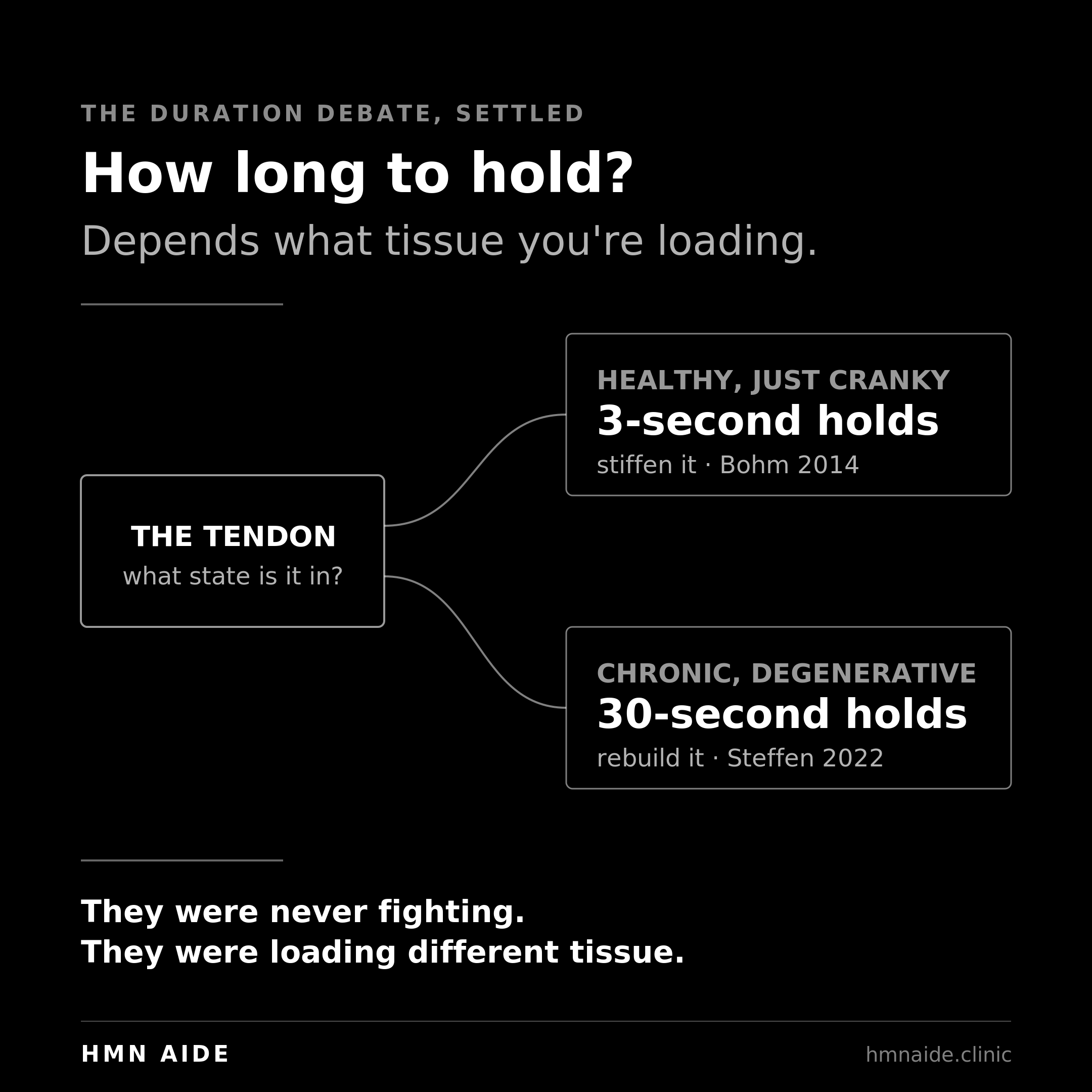
Hold duration looked like a fight between good labs until you sort it by which tissue you're loading. For a healthy tendon you're trying to stiffen, short wins: the Berlin lab's own head-to-head beat 12-second holds with 3-second holds. For a degenerative scar, long wins: in scarred tendon, 30-second isometric holds drove regeneration markers while the exact same time under tension delivered as fast reps pushed the tendon toward fibrocartilage instead. So it isn't 3 versus 30 in the abstract. It's 3 for a tendon that's basically fine and you want stiffer, 30 for a tendon with a degenerative core you're trying to rebuild. That second half is rat data plus one human case, so hold it loosely. But the logic routes cleanly, and the two camps were never really fighting. They were loading different tissue.
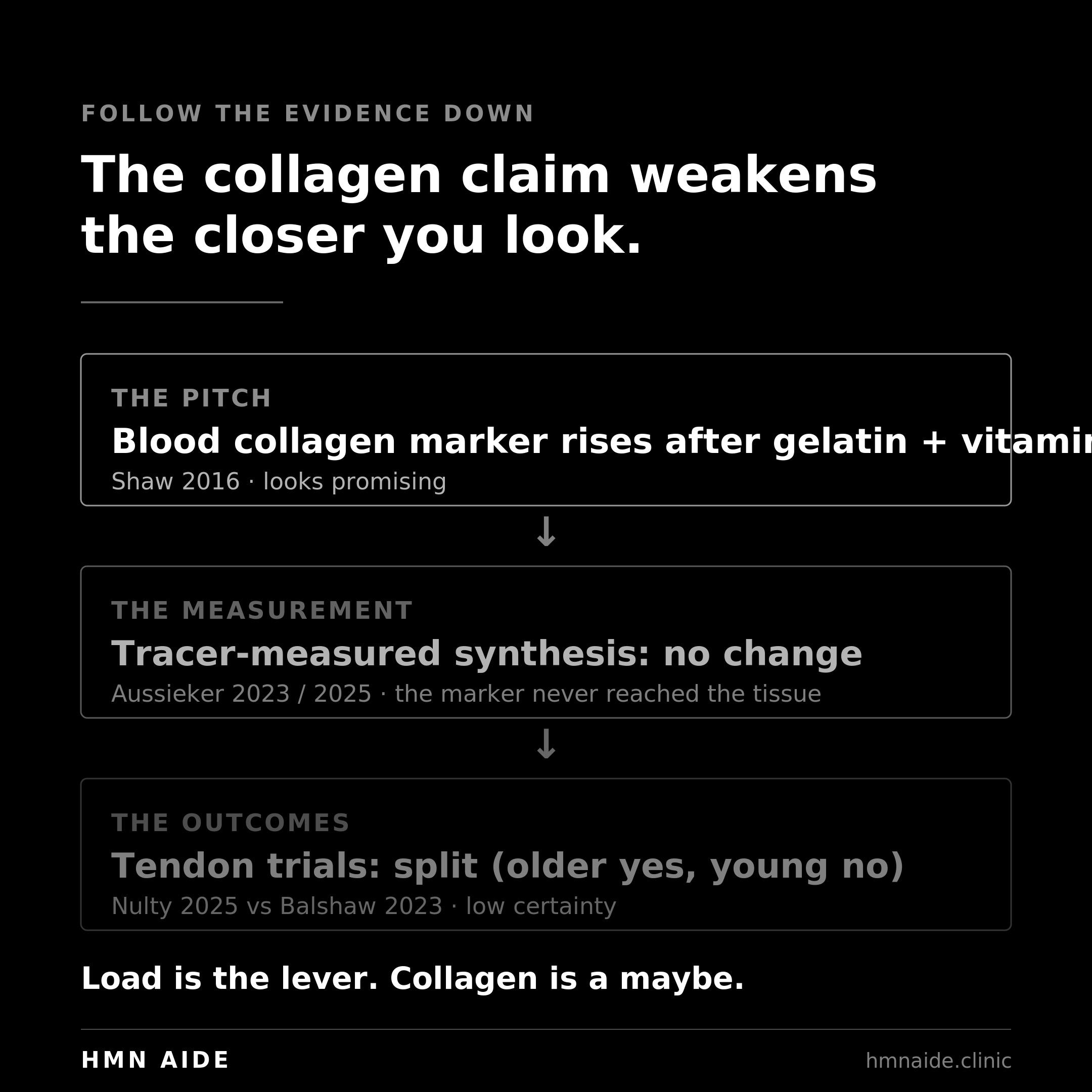
Accelerants beyond load are mostly hype, and the one people are most excited about deserves more skepticism than it gets. Collagen is a garbage protein by the usual standard. Incomplete, low in leucine, basically no tryptophan, so it does almost nothing for muscle protein synthesis. The argument for it was never about that pathway. It's that collagen is packed with glycine and proline, the raw material a tendon cell needs to build new collagen, which ordinary high-quality protein is short on. Take gelatin and vitamin C before you load and the collagen-building signal in your blood goes up. Plausible enough. But when researchers stopped trusting the blood marker and measured actual synthesis with isotope tracers, the cleanest data we have, taken in muscle connective tissue, collagen did not raise connective-tissue protein synthesis, and neither did free amino acids matched to collagen's own profile. The glycine showed up in the blood and did nothing you could measure in the tissue. The tendon-outcome trials are split on top of that: 30 grams helped middle-aged men over 12 weeks, 15 grams did nothing for young men. And the famous case of a tendon normalizing on MRI with gelatin and stress-relaxation holds is one professional basketball player. So the honest read is weak and conditional. Maybe worth it if you're older and the tissue is lagging, cheap and safe enough that trying it costs little, not the lever the hype makes it. Load is the lever. Collagen is a maybe.
And the scan. Stop chasing it. Structure on imaging does not track pain. People get better while the tendon still looks ugly on ultrasound, and tendons look ugly in people with no pain at all. A 2026 study found no imaging feature predicted who'd improve. Even Cook, whose staging model the whole rehab world runs on, walked it back and admitted you can't stage a pain problem off structure. The picture is not the patient.
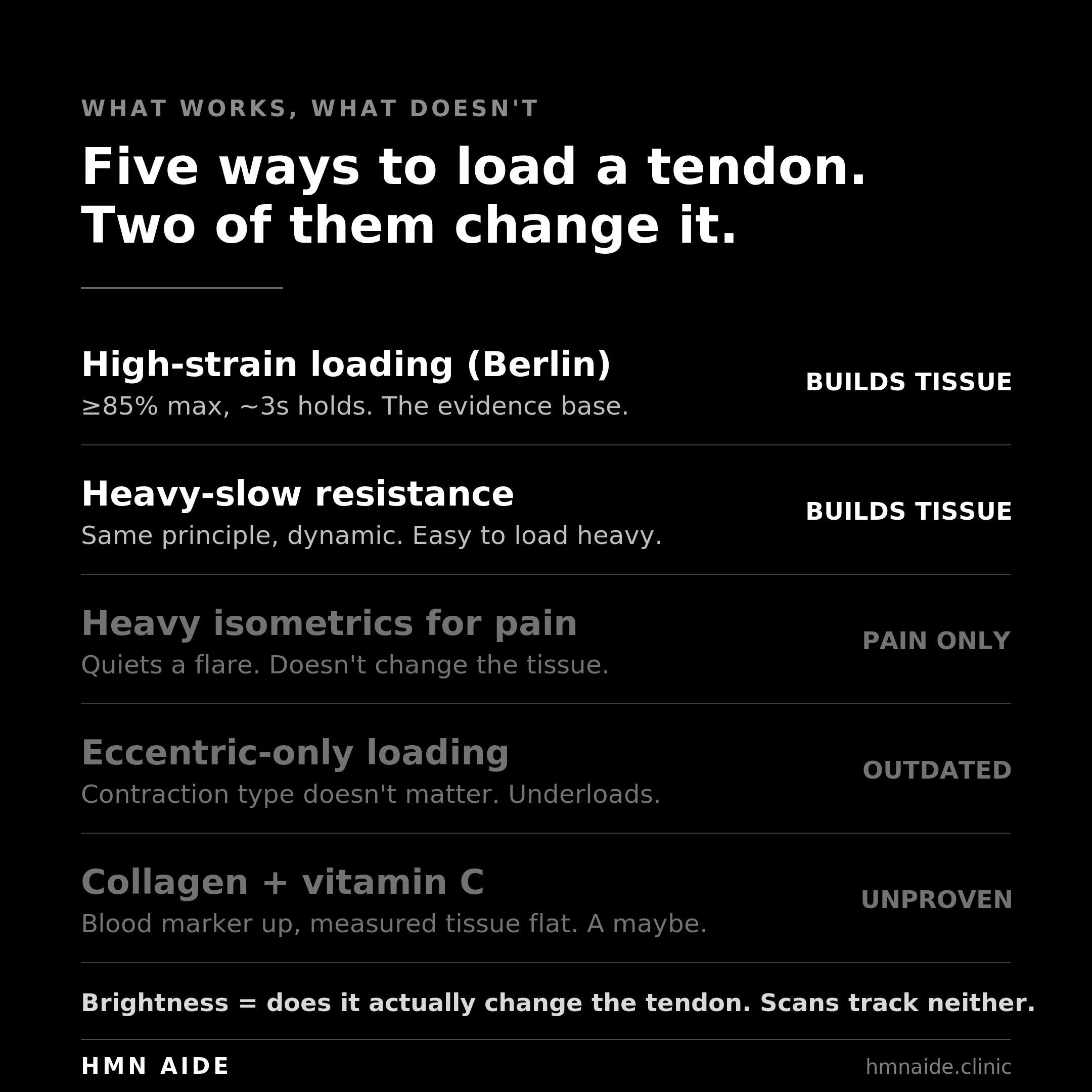
Protocol What it's for The number Verdict Heavy isometrics for pain Quieting a flared tendon short-term 45s holds, high load Works as pain relief, not tissue change. Not special vs other contractions. Eccentric-only loading The old default Slow lowers, "to tolerance" Outdated. Contraction type doesn't matter. Often underloads. Berlin / high-strain loading Actually remodeling the tendon >=85% max, ~3s, 5x4, 4x/wk, 12+ wks The evidence base. Builds stiffness and capacity. Heavy-slow resistance Tendinopathy strength rebuild Heavy load, slow tempo, ~3x/wk, symptom-guided, pain <=3/10 settling in 2-4h Solid. Same principle, just dynamic. Easier to load heavy. Collagen + vitamin C Adjunct, not a driver ~15-30g + 50mg C, 1h pre-load Promising for older/lagging tissue. Null in young. Low certainty. Imaging / scans Ruling out red flags only — Useless for tracking progress. Doesn't track pain.
So before you read one more thing about it, here's the move to do today. Find the position that loads the sore tendon the hardest without the pain climbing past a 3. For an Achilles, that's a single-leg calf raise held hard at the top, knee straight. For the front of the knee, a wall sit or a split-squat held dead still at the depth where the kneecap tendon switches on. Anywhere else, load the muscle that pulls on the sore spot and hold it there. Push like you mean it, about as hard as you'd grip to stop a door from slamming, and hold five seconds. Five of those. The pain is allowed to touch a 3 and it has to be gone by tonight. If it spikes, or it's still loud tomorrow, you went too heavy, go lighter and try it again. Your only readout is whether you can load it harder with less pain over the coming weeks. Never the scan.
What that one set won't tell you is how many to do, how many days a week, how to add load without lighting it up, and how long until you're springing off it again. It won't tell you whether yours is the healthy-but-cranky tendon that wants short hard holds or the chronic, degenerative kind that wants long ones. And it won't tell you whether collagen is worth your money or a waste of it for a body like yours. That's the twelve-week build, and it's the part that actually turns the tissue over. One honest rep today is the on-ramp. The dosing over three months is the road.
The tendon reads one number. Give it that number, often enough, for long enough, and stop negotiating with it about everything else.
This article is educational and not a substitute for medical advice. Consult a qualified professional before making decisions about your health.
Sources
Rio E, Kidgell D, Purdam C, et al. 2015. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. British Journal of Sports Medicine 49(19):1277-1283. (The original isometric-analgesia finding; n=6 crossover.)
Rio E, van Ark M, Docking S, et al. 2017. Isometric contractions are more analgesic than isotonic contractions for patellar tendon pain. Clinical Journal of Sport Medicine 27(3):253-259. (The n=20 follow-up; the second of the two studies the trend rests on.)
van der Vlist AC, et al. 2020. Isometric exercises do not provide immediate pain relief in Achilles tendinopathy. Scandinavian Journal of Medicine & Science in Sports 30(9):1712-1721. (n=91, four arms including rest; no immediate analgesia.)
Holden S, Lyng K, Graven-Nielsen T, et al. 2019. Isometric exercise and pain in patellar tendinopathy: a randomized crossover trial. Journal of Science and Medicine in Sport 22(12):1320-1325. (0.9/10 pain change, isometric no better than dynamic.)
Clifford C, Challoumas D, Paul L, et al. 2020. Effectiveness of isometric exercise in the management of tendinopathy: a systematic review and meta-analysis. BMJ Open Sport & Exercise Medicine 6(1):e000760. (Isometric not superior to isotonic.)
Challoumas D, et al. 2021. Management of patellar tendinopathy: a systematic review and network meta-analysis. BMJ Open Sport & Exercise Medicine 7(4):e001110. (Isometric as effective, not more, than isotonic for immediate pain relief.)
Riel H, Vicenzino B, Jensen MB, et al. 2018. The effect of isometric exercise on pain in individuals with plantar fasciopathy. Scandinavian Journal of Medicine & Science in Sports 28(12):2643-2650. (Isometrics no better than isotonics or walking; the plantar-fascia tie.)
Arampatzis A, Karamanidis K, Albracht K. 2007. Adaptational responses of the human Achilles tendon by modulation of the applied cyclic strain magnitude. Journal of Experimental Biology 210(15):2743-2753. (The within-subject strain-threshold study: only the high-strain leg adapted.)
Bohm S, Mersmann F, Arampatzis A. 2015. Human tendon adaptation in response to mechanical loading: a systematic review and meta-analysis. Sports Medicine - Open 1:7. (27 studies; loading magnitude drives adaptation, contraction type does not.)
Bohm S, Mersmann F, Tettke M, et al. 2014. Human Achilles tendon plasticity in response to cyclic strain: effect of rate and duration. Journal of Experimental Biology 217(22):4010-4017. (Head-to-head 3s vs 12s; the 3s reference protocol produced higher stiffness gains.)
Kubo K, Kanehisa H, Ito M, Fukunaga T. 2001. Effects of different duration isometric contractions on tendon elasticity in human quadriceps muscles. Journal of Physiology 536(2):649-655. (Long holds built more stiffness than short in a healthy tendon; part of the duration picture.)
Steffen D, Avey A, Mienaltowski MJ, Baar K. 2022. Scleraxis and collagen I expression increase following pilot isometric loading experiments in a rodent model of patellar tendinopathy. Matrix Biology 113:1-13. (Direct head-to-head in scarred tendon: long 30s isometric holds drove regeneration markers, TUT-matched dynamic loading drove fibrocartilage. The hold-duration routing answer.)
Arampatzis A, Peper A, Bierbaum S, Albracht K. 2010. Plasticity of human Achilles tendon mechanical and morphological properties in response to cyclic strain. Journal of Biomechanics 43(16):3073-3079. (Low strain frequency, the 3s/3s rhythm, outperforms high frequency.)
Malliaras P, Barton CJ, Reeves ND, Langberg H. 2013. Achilles and patellar tendinopathy loading programmes: a systematic review. Sports Medicine 43(4):267-286. (Evidence for heavy-slow resistance in patellar tendinopathy; the basis for the HSR row.)
Arampatzis A, Mersmann F, Bohm S. 2021. The "Berlin method": practical recommendations for tendon training. Humboldt-Universitat zu Berlin. (Primary source for the protocol: >=85% MVC, ~3s, 5x4, 4x/week, 3+ months. Verifies/corrects the softened figures in circulation.)
Nulty CD, et al. 2025. Hydrolysed collagen supplementation enhances patellar tendon adaptations to 12 weeks' resistance training in middle-aged men. European Journal of Sport Science. (30g collagen added tendon CSA/stiffness/modulus over placebo in middle-aged men.)
Balshaw TG, et al. 2023. The effect of specific bioactive collagen peptides on tendon remodeling during 15 wk of lower body resistance training. Medicine & Science in Sports & Exercise 55(11):2083-2095. (15g collagen, no tendon benefit beyond training in young men. The null half of the collagen picture.)
Shaw G, Lee-Barthel A, Ross ML, et al. 2016. Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis. American Journal of Clinical Nutrition 105(1):136-143. (The blood-marker mechanism: gelatin + vitamin C before loading raises a circulating marker of collagen synthesis.)
Holwerda AM, van Loon LJC. 2021. The impact of collagen protein ingestion on musculoskeletal connective tissue remodeling: a narrative review. Nutrition Reviews 80(6):1497-1514. (The rationale is substrate, glycine/proline, not muscle protein synthesis.)
Aussieker T, et al. 2023. Collagen protein ingestion during recovery from exercise does not increase muscle connective protein synthesis rates. Medicine & Science in Sports & Exercise 55(10):1792-1802. (Isotope-tracer measurement: 30g collagen did not raise connective-tissue synthesis.)
Aussieker T, et al. 2025. Hydrolyzed collagen versus free amino acids on muscle connective protein synthesis rates. Medicine & Science in Sports & Exercise. (Neither collagen nor collagen-profile free amino acids raised connective-tissue synthesis despite raising plasma glycine.)
Baar K. 2019. Stress relaxation and targeted nutrition to treat patellar tendinopathy. International Journal of Sport Nutrition and Exercise Metabolism 29(4):453-457. (The MRI-normalization result; a single professional basketball player. n=1 case study.)
Cook JL, Purdam CR. 2009. Is tendon pathology a continuum? British Journal of Sports Medicine 43(6):409-416. (The staging model the rehab field runs on.)
Cook JL, Rio E, Purdam CR, Docking SI. 2016. Revisiting the continuum model of tendon pathology. British Journal of Sports Medicine 50(19):1187-1191. (The authors' own walk-back: you can't stage a pain condition off structure.)
Deng J, et al. 2026. Prognostic value of conventional ultrasound and MRI features for clinical outcomes in athletes with patellar tendinopathy after exercise therapy. Sports Health. (No imaging feature predicted 24-week pain or disability change.)